Comments:
The vaginal hysterectomy is the least invasive method of removal of the uterus. Most of the hysterectomies may be performed vaginally.The lower rate of the vaginal hysterectomy is not only due to the relative contraindications to the vaginal route of the hysterectomy but also due to the technical barriers in the mind of most surgeons to deal with inadequate accessibility, poor visibility, and effective hemostasis even after considerable experiences.That is why they prefer a more obvious and widely visible abdominal or laparoscopic route of the hysterectomy even for a moderate size uterus.Our goal should be to perform the vast majority of hysterectomies for benign disease via the vaginal route. Only detachment of the lateral attachments was enough to remove the uterus in majority (86.45%) of cases. Debulking was needed in only 13.55% cases when Purohit technique was used. Failure is very rare(<1%).
We have performed over 10000 vaginal hysterectomy by Purohit technique ( PTVH).
How to achieve adequate visibility during vaginal hysterectomy.
Enhancement of visibility increases the feasibility, safety, efficiency, and satisfaction of the surgeon. We feel enhancement of visibility is more important than the type of speculum and retractors used. Use thin and long(22cms) instruments to improve passage of light in to the operation field. Use few instruments (right-angle forceps, bipolar forceps, and scissors). Do not dissect by fingers. It obstructs vision. Do not use thick clamps obstructing vision.Do not use sutures to ligate a stump. A thin (2 mm tip) long bipolar forceps may be enough for hemostasis. Do not use hand to apply knots. It obstructs vision. A pelvic illuminator or a 10 mm used telescope with light source is enough to increase the visibility of vaginal canal and lateral pelvic wall structures. A pelvic illuminator offers the advantages of a long (18 inches) rigid thin torch that can be directed to a deeper and darker part of pelvic cavity precisely from a required angle. It helps visualizing structures up to the level of infundibulopelvic ligament during salpingo oophorectomy. It is handled either by the left or right assistant. However, a telescope or a pelvic illuminator with the light source is required in about 10% cases of the vaginal hysterectomy, and more frequently when salpingo oophorectomy is desired. It is of distinct advantage in localizing precisely the bleeder from the lateral wall after removal of the uterus. We believe a surgeon equipped with operative laparoscopic set up can expand the limit of feasibility of the vaginal hysterectomy. We have devised a special pelvic illuminator(Dr R K Purohit pelvic illuminator) consists of a 10 mm rigid tube containing only optical fibres.It has a handle at one end. Length is about 18 inches. It does not contain any lens thus it is cheaper. Now, the overhead operation theater LED light has solved many of above difficulties of visibility in the deeper field of the vaginal hysterectomy.
Incision of anterior vaginal wall by monopolar current
Incision on the anterior vaginal wall is given by a frequent gentle stroke sufficient to expose the wall of the cervix. A deeper incision will incise the superficial part of myometrium and will go beyond the line of cleavage. It will resemble a strong band of adhesion in the midline and will cause dissection problem. Little superficial incision, on the other hand, will fall short of reaching the line of cleavage. Forceful dissection through this wrong plane will hit the bladder wall and will result in penetration of lumen of the bladder. (The modified method, described in the operation procedures eliminates the problems of finding cleavage.) The anterior margin of incision is lifted by an Alli's forceps when the incision falls short of the line of cleavage.The stretched taught tissue between the cut margins (the supravaginal septum or vesicovaginal septum) is gently incised by a curved scissor directing its curvature against the anterior wall of the cervix to get the cleavage to enter to the vesicocervical space. When the incision goes beyond the line of cleavage, the adhered superficial layer of cervix to anterior incision is treated as a strong band of adhesion and dissected later on by a lateral approach of right-angle forceps. Moreover, the complex anatomy around the uterine cervix needs a systematic approach to prevent most complications.
Dissection of vesicocervical space and separation of the bladder from the cervix.
Vesicocervical space is bounded anteriorly by the bladder, posteriorly by the uterus and cervix, laterally by bladder pillars, below by supravaginal septum and above by vesicouterine peritoneum. It contains the loose fascia. Normally the bladder is peeled easily and quickly from the cervix by finger dissection. If adhesions are sensed by finger during dissection, they are divided by sharp dissection. Dissection is stopped on sensing a strong band of adhesion. No strong force is applied to detach it. Usually, these bands are thin and found in the lower boarder of vesicovaginal space. The space above the scar is soft and can be easily pushed by finger. By a lateral approach, the finger is pushed lateral to the scar band to reach the upper part of the vesicocervical space.The upper space is dissected by medially bend index finger and the band is isolated. It is then 'hooked' by the finger.We prefer to 'hook' it by the bend of a right-angle forceps (Figure 1) in the place of the index finger.It increases visibility.The tip of the right-angle forceps is placed just above the stump of ascending branch of uterine artery.The tip is moved gently medially to push it in to the uterovesical space.It hooks the supravaginal septum or uterovesical scar in a case of previous CS.The jaws are opened to stretch the septum.It is separated from the lateral aspect and from the edge of the uterus to avoid bladder injury.The other half is separated by a similar procedure from the opposite side.
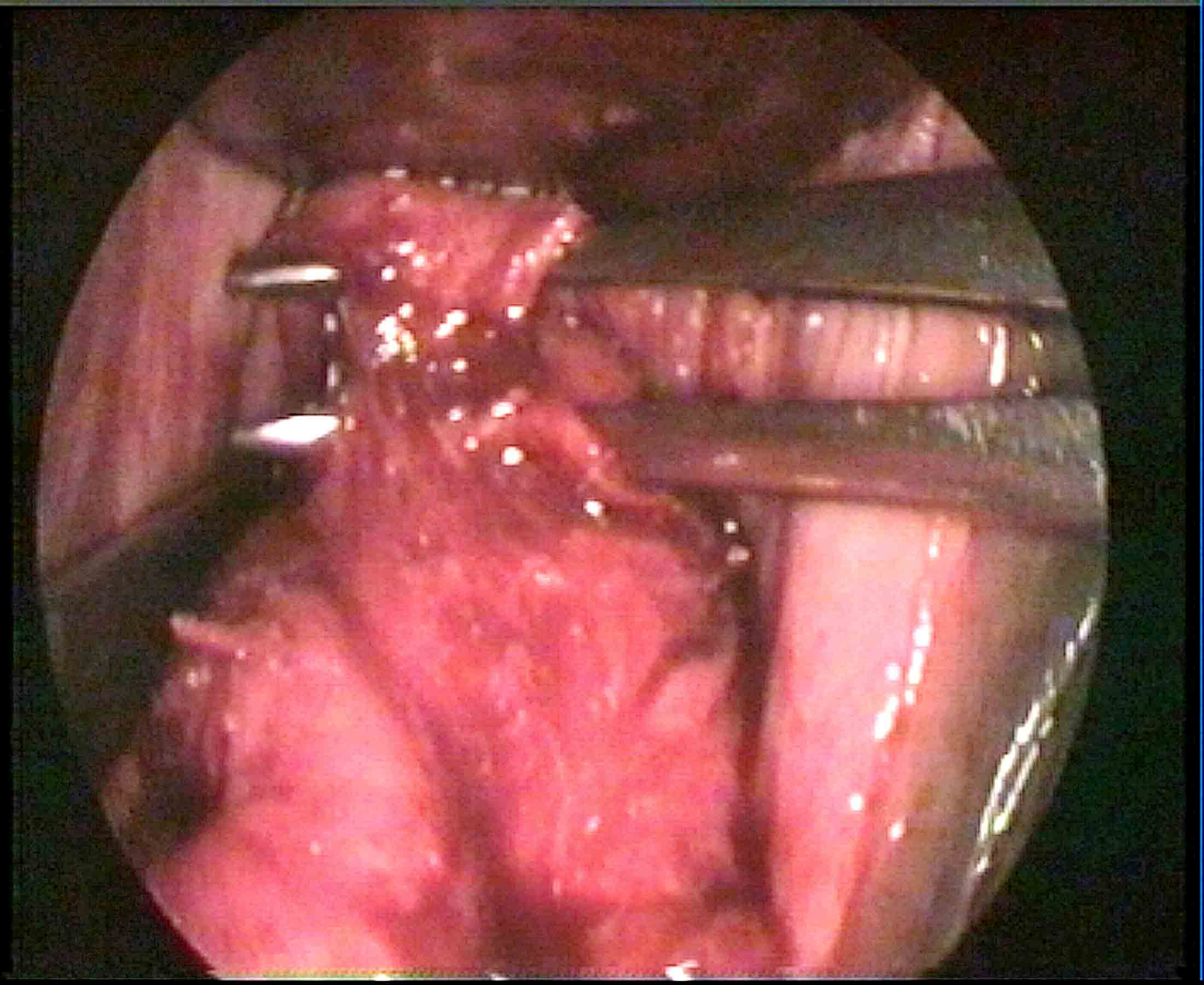
Figure - 1
The above procedure is applied to the very thick and wide band of adhesion covering the whole width of the anterior wall of the cervix between bladder pillars.
Conventional technique using ligatures
for hemostasis requires three steps (clamping, cutting and suture ligation) , many instrument changes and a wide space for the movement of a curve needle on a holder, where as, the newer techniques of hemostasis using bipolar energy, ultrasonic energy and electro thermal bipolar vessel sealer (EBVS), plasma kinetic energy, etc. require two steps (coagulation- and -cut) fewer instrument changes, and less space for a thin forceps. The space required by a needle for its movement is eliminated. Bipolar coagulation by ordinary bipolar forceps with the fine tip, may, at least be used in place of the traditional ligature method.It is available in a standard operation theatre, cheap and safe in the vaginal hysterectomy. Coagulation -and -cut maneuvers will shave the uterus from its natural lateral attachments and adhesions precisely.Use of a right-angle forceps as in Purohit technique, radically, solves the question of inaccessibility to vesicocervical- cardinal- uterosacral ligaments, even, in cases with very poor access. It acts as a helper. It elevates the cervix from the posterior aspect by the tip and brings the ligaments to surgeon’s view.It creates a narrow working platform between its opened prongs sufficient for bipolar forceps and scissors and keeps the neighboring tissues away. The working platform between the opened prongs of right angle forceps increases the safety. All energy- based forceps (bipolar energy, ultrasonic energy and electro thermal bipolar vessel sealer (EBVS)plasma kinetic energy, etc.) may use this platform to reduce the complications due to spread of energy. Bipolar forceps always occupies less space than other forceps like bi-clamp and harmonic.Opening of posterior Pouch:
It is easier to access the posterior pouch than the anterior pouch by various techniques. The problem arises when the pouch cannot be opened due to dense adhesion, endometriosis, or when it is highly placed due to posterior cervical myoma. Extraperitoneal uterosacral ligament separation, uterine artery ligation, separation of adhesions close to the uterine wall, and intracapsular morcellation of cervical fibroid enhance the descent of the uterus.Then, the anteroposterior approach is done through the anterior cul-de-sac(reference no 7).The wall of the rectouterine adhesions in endometriosis is then separated by tactile feel of the index finger.Nowadays, the vaginal hysterectomy can be done in cases of the obliterated posterior cul-de-sac.The posterior leaf of the broad ligament is then hooked by the bend of right angle forceps,coagulated and divided. Adhesions in the pouch are easily hooked by the bend of right-angle forceps as in Purohit technique and plucked one by one. It is easier than the inconvenience caused by the wide space requiring ligature method of hemostasis. Fiber optic rigid light source often increases visibility.
Choice of forceps with energy for vaginal hysterectomy
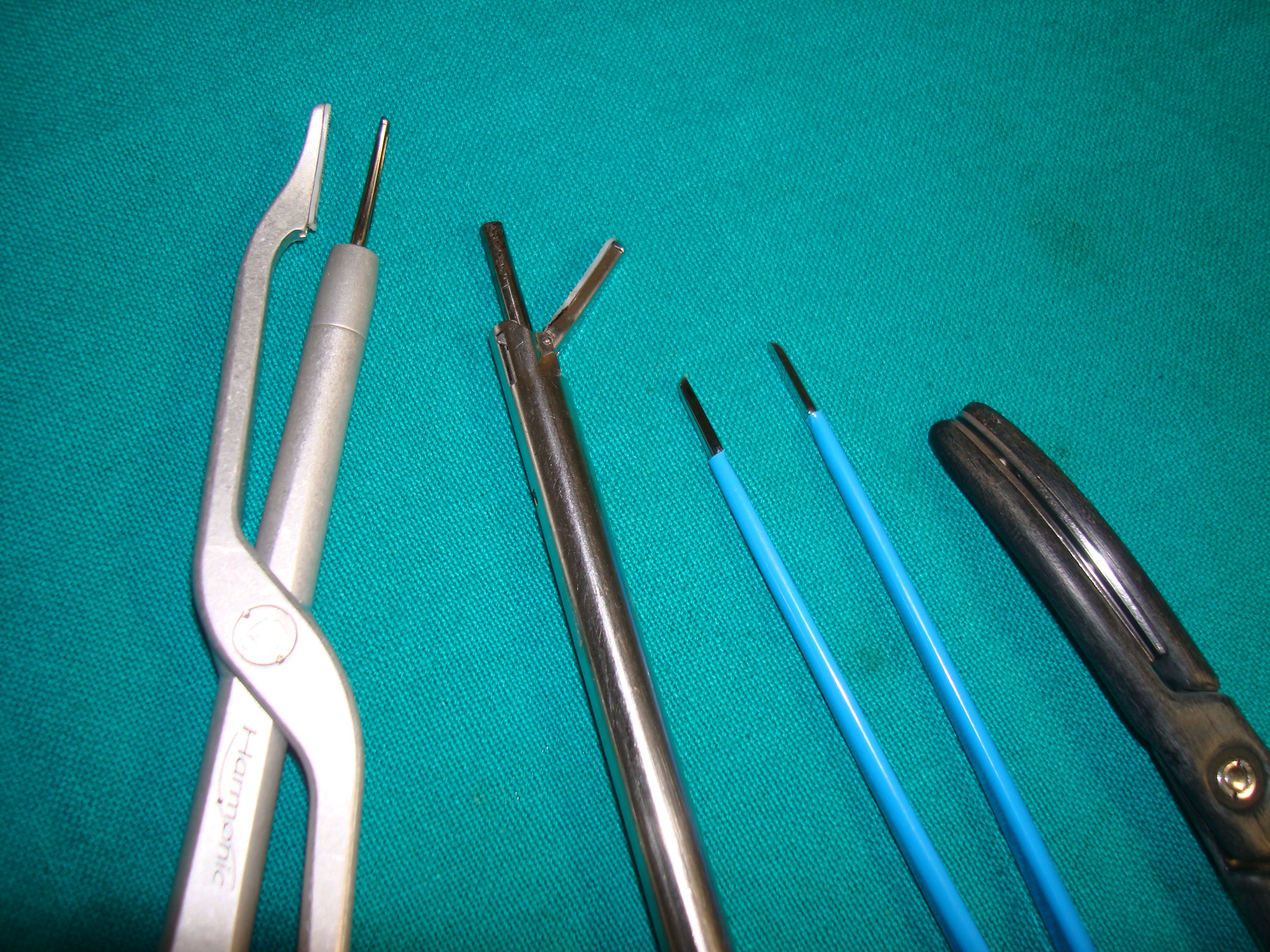
Figure 2 (compares thickness of tips of forceps)
Bipolar forceps alone may be used throughout.It has the thin tip. Bipolar forceps may be combined with Bi clamp forceps. Use bipolar forceps up to the level of the uterosacral ligament and uterine artery. Above level of the uterosacral and uterine artery we get wider space, and then, use bi clamp.Bi clamp has the thick tip. At the end, we again use bipolar forceps for effective hemostasis of tiny vessels. Similarly, we use thick Harmonic (focus and wave) forceps when the available space is wide. Scissors is usually not needed when Harmonic focus is used. Postoperative pain is less in cases after the harmonic than after bipolar. Similar to bipolar forceps, three strokes of harmonic forceps (at level -1 setting) along the length of the uterine artery seals the uterine artery stump. We keep bipolar forceps ready in case harmonic does not seal the vessel. now, we are using bipolar sealer cum divider.It seals and divides.It is a short (18cm) version of laparoscopic forceps.It is good for all purposes. However, all forceps are used between prongs of right-angle forceps to improve the safety and success of the vaginal hysterectomy(Figure 3)
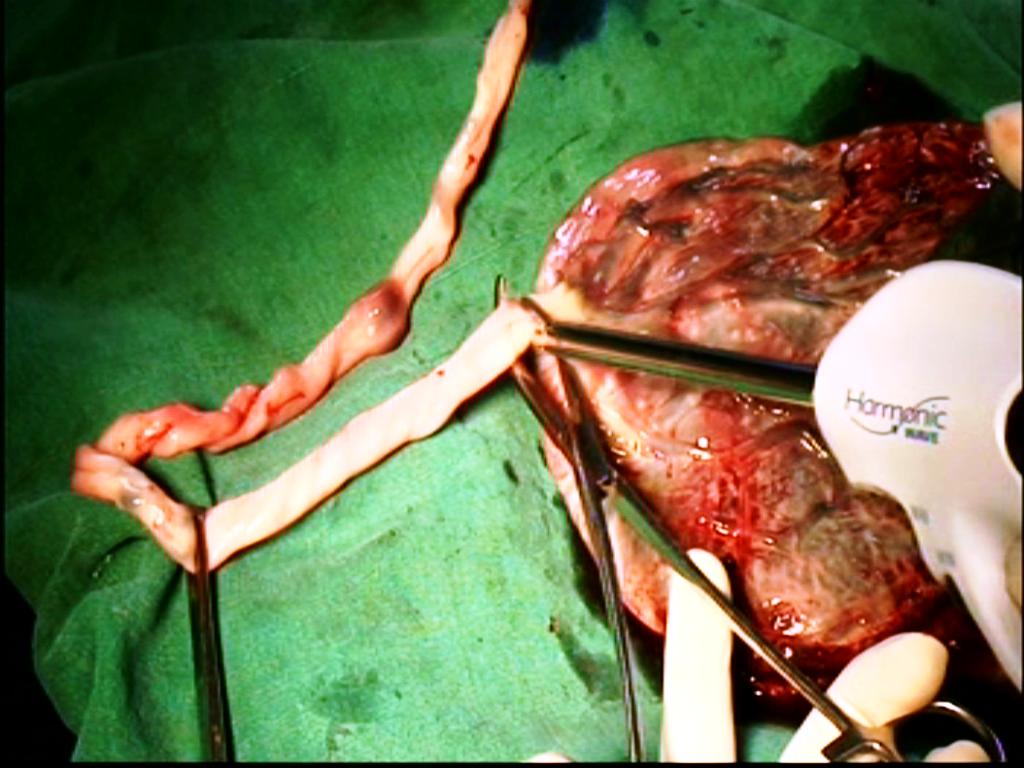
Bipolar,Bi clamp and Harmonic wave -placenta Model
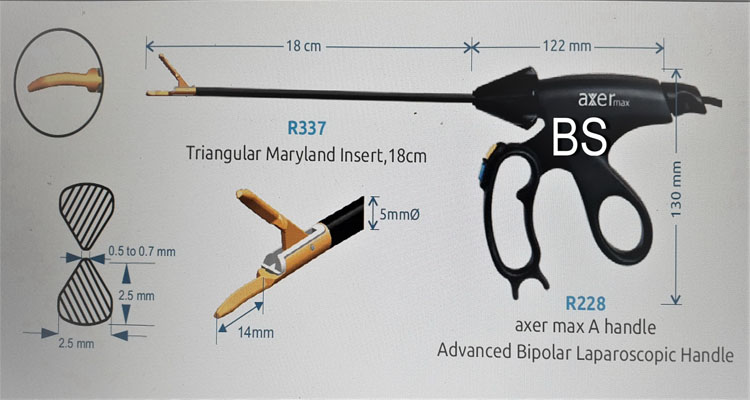
Photo of bipolar sealer/cutter
Detachment of adhesions.
The uterus can be detached from all the lateral adhesions, and the hysterectomy can be completed. It is easier and quicker by using the modern methods of hemostasis than by the ligature methods of hemostasis. A right-angle forceps is of great help in 'hooking' the adhesions. It works like a bend index finger during the operation. It is almost not possible to detach vaginally the rarely found plastic adhesion of the uterine fundus to the anterior abdominal scar (ventrofixed uterus) resulting from the previous cesarean section. In a case of adhesion with bowel loop, a slice of serosa of the uterine wall is spared. We have an experience of failure to detach vaginally, a thick wide adhesion of fundus of a normal size uterus to a suprapubic transverse anterior abdominal scar following previous CS, and following previous minilap tubal ligation operation. In another case of the previous cesarean section, the whole of the anterior surface of the uterus was adhered to the anterior abdominal wall scar(ventrofixed uterus). Both required laparoscopic assistance at the end to complete the vaginal hysterectomy. Ventrofixed uterus to be excluded in all cases with the previous cesarean section.It is better not to attempt such ventrofixed cases vaginally (contraindication).
How to suspect clinically the fundal adhesion to the anterior abdominal wall scar following previous CS(ventrofixed uterus).
Figure 4 Fundal adhesion to anterior abdominal wall.
Ordinarily, the cervix is visible on office speculum examination. In a case of the previous cesarean section, when the cervix cannot be easily seen on speculum examination, and it can only be seen with great difficulty with the help of an anterior wall retractor, or when the cervix cannot be easily palpated on bimanual examination, but with difficulty at a height behind the symphysis pubis. When the traction of cervix by tenaculum causes a depression on the anterior abdominal wall scar over the site of adhesion. Backward and upward movement of a uterine sound in the uterine cavity under anaesthesia causes a depression of the anterior abdominal wall scar at the site of fundal adhesion(uterine sound retroversion test-reference no 8). It is done in a case of previous CS just before starting vaginal hysterectomy to exclude ventrofixed uterus.
How to achieve effective hemostasis during vaginal hysterectomy
At the vesicocervical- cardinal- uterosacral ligaments:
Traditionally ligaments are clamped, detached, and transfixed by suture when space is wide.The ends are held long for fixation to the vault at the end of the operation.The clampless technique is practiced when the space is inadequate. Use of a thick clamp, insertion of a curve needle lateral to the upper end of the clamp and needle retrieval from the posteriolateral aspect of the thick clamp require a wide space.It is troublesome when space is still inadequate. Moreover, a chance of ligature slippage causes apprehension of bleeding.In Purohit technique, ligaments are shaved from the edge of the cervix after bipolar coagulation (coagulation -and -cut maneuvers). It reduces chances of hemorrhage and ligature slippage.Ligaments are approached extraperitoneally.Tip of a right-angle forceps is used to elevate the cervix from the posterior aspect to bring the target tissue to the operator's view before coagulation and division.The coagulation -and -cut maneuvers need about 4 mm space.Thus, this technique is helpful in all cases with poor access.In our experience, lower ligaments of all cases with benign disease of the uterus can be detached by Purohit technique.The forceps used in the modern techniques of hemostasis like bipolar and harmonic etc need a straight passage to the target organ and thus require less space than the curve passage used by the ligature technique of hemostasis.When other forceps fail, bipolar forceps works thus, always keep the bipolar forceps during the vaginal hysterectomy.In Purohit technique, utilisation of a right angle forceps further increases safety of the neighboring structures.Traction by the assistant is not so much required in our technique because tip of right-angle forceps is used by left hand to elevate the ligaments from the posterior aspect for easy application of bipolar forceps by right hand.That reduces the tiredness of the assistant and postoperative pain of the patient.The released Mackenrodt's ligament does not retract back in any case, in this extraperitoneal technique.We found, that the difficulty of application of the thick clamp and needle holder with the needle in such cases of poor access in conventional method could be solved by our technique.Therefore, cases with poor access were not a contraindication in our technique.
How to achieve hemostasis of uterine arteries
Correctly, applied ligature is a time tested reliable method of hemostasis if the space is wide for ligature application.Clamp less technique used when the space is inadequate.When the space is still narrow then the modern hemostatic techniques like bipolar energy,ultrasonic energy, electrosurgical bipolar vessel sealer (EBVS) are used. When the distance between the ureter and cervix is 0.5 cm then the chance of ureteral injury relatively increases during hysterectomy.Isolation of uterine artery rather than bundle inclusion is a vital step to avoid coagulation injury to the neighboring structure.Purohit technique is different specially in showing advantages of use of a right angle forceps in isolating the uterine artery extraperitoneally. The right angle forceps creates space for bipolar forceps and scissors between its opened prongs and protects the neighboring structures from thermal injury.In this extraperitoneal technique, a bleeding uterine artery protrudes towards the surgeon than it retracts.A bleeding artery can be easily grasped by artery forceps and cauterized extraperitoneally.In this intraperitoneal technique, blood does not enter in to the peritoneal cavity during the procedure and bowels do not protrude on to the operation field.In the intraperitoneal technique in contrast, blood enters the peritoneal cavity, bowels come on the way of operation, the lower ligament, and uterine artery stumps recoil back to the lateral pelvic wall immediately after separation from cervix and uterus.It is some time difficult to trace a bleeding uterine vessel in the intraperitoneal approach to uterine artery.In our experience, uterine arteries can be secured extraperitoneally bilaterally in all cases of benign disease of uterus up to 16 weeks size of gestation.We have not encountered a case of postoperative hemorrhage from uterine artery.We believe bipolar method of hemostasis is reliable, safe, effective, and cheap in vaginal hysterectomy.Achievement of complete physical compression of the lumen (coaptation) of artery by prongs of bipolar forceps is a prerequisite before activating bipolar current.Bipolar needs 2-3 applications along the length of uterine vessel for complete hemostasis. We have not seen an avulsed stump postoperatively. Purohit approach to uterine artery is an easier and quicker approach to access, identify, dissect,and skeletonise the uterine artery even in cases of rotated and distorted uterus due to myoma.Its desiccation under direct vision between the prongs of right angle forceps further increases confidence and reduces intraoperative hemorrhage and chances of injury to ureter.
How to achieve hemostasis of the upper pedicles
Traction is given on the round ligament stump and all the stumps are exposed.The bipolar method of hemostasis is also reliable for the upper pedicles.Bipolar forceps is preferable in cases with narrow lateral space resulting from expanded uterine fundus and pelvic adhesions.Pelvic illuminator may be used in cases with poor visibility.
How to check effective intraoperative hemostasis during vaginal hysterectomy by electrosurgery
In Purohit technique, posterior leaf of broad ligaments is routinely climbed up/traced bilaterally up to the infundibulopelvic ligament to trace bleeder if any from the lateral wall to prevent postoperative vault hematoma.Intraoperatively bleeding occurs from three sites: (1) from the veins and arterioles of Mackrnodt's ligament (2) from the ovarian pedicles and occasionally from a tiny vessel below round ligament(artery to round ligament),and (3) from the uterine artery.To deal with the bleeding from upper pedicles, trace the pedicles by the technique described above, pull them down, and coagulate them properly.Use pelvic illuminator, if needed to improve visibility.To deal with the uterine artery bleeding, trace it by the tracing technique described above.Use the pelvic illuminator, if needed to improve visibility.Then, hold the bleeding stump by an artery forceps.Use suction cannula to aspirate the blood. Lavage with normal saline.Now, cauterize the artery proximal to the artery forceps.Well-cauterized artery is reliable postoperatively.Do not use suture or do not mix suture and bipolar.For bleeding from Mackrnodt's ligament, hold the lateral vaginal wall by Allis forceps, pull it laterally to find any bleeding artery, and cauterize it.In the absence of arteriolar bleeding, retrieve the uterosacral stump, and then fix it to the lateral vaginal wall.It will compress and stop the venous bleeding that cannot otherwise be cauterized.No time is wasted in catching the venous bleeding from in side the ligament tear.Primary postoperative bleeding, if any from the lateral wall can also be traced and secured by this technique safely after opening the vaginal vault without affecting security of other stumps.
Salpingo oophorectomy at the vaginal hysterectomy(Purohit technique)
Separation of the round ligament from the ovarian ligament with the tube as in abdominal hysterectomy is a prerequisite to reach the infundibulopelvic ligament in vaginal salpingo oophorectomy. It is more anatomical than bunch inclusion of all pedicles. Suture transfixation, stapling, and Roeder's loop application have been the methods of hemostasis to occlude the ovarian vessels. Inadequate space caused difficult suture ligation and chances of ligature slippage. Taking the advantages of the use of a right-angle forceps as in Purohit technique, salpingo oophorectomy can be done in almost all indicated cases. It elevates the infundibulopelvic ligament from posterior aspect, brings it to surgeon's view, and creates a working space between its prongs for bipolar forceps and scissors. It retracts and protects the neighboring structures. Postoperative security of the ovarian vessels is reliable after bipolar cauterization. Pelvic illuminator frequently improves the visibility in difficult cases. A standby operative laparoscopy facility increases the confidence of the surgeon. Adhesions are dissected by right angle forceps. All benign movable ovarian cysts, tubo-ovarian mass, chocolate cyst with minimal adhesions can be removed by this technique.Larger cysts are aspirated by suction aspiration using a long Verses needle to increase working space. Dense benign adhesion of ovary to upper pelvis and endometriotic adhesion of the ovary to the upper pelvis, in our experience should not be attempted vaginally.The vaginal attempt usually fails. It needs laparoscopic assistance or minilaparotomy after vaginal extraction of the uterus. Laparoscopic salpingo oophorectomy at this stage is easier and takes less time. It is initiated from stump side than the infundibulapelvic ligament side. The vaginal vault is clamped by three Alli's forceps horizontally to reduce gas leak. The excised tube and ovary are removed vaginally.Now, adhered adnexa to pelvic sidewall can be mobilised by transvaginal manual mobilisation technique before adnexectomy(Reference no 6)
Purpose of debulking of large uterus
Normal size uterus generally does not obstruct the accessibility to lateral pedicles. An enlarge uterus fills the pelvic cavity centrally and compresses drastically the lateral working space. It obstructs to the visibility and accessibility to the lateral pedicles to be secured. All lateral attachments of uterus are separated from the body to accomplish removal of uterus. Therefore, removal of the bulk is essential to increase the lateral space. Debulking is initiated when no further lateral pedicle is 'hooked' on sweeping the tip of forceps around the expanded lateral wall of uterus.
The feasibility of debulking
Uterus, larger than 12-14 weeks size invariably requires a debulking. Only, 10-15 % of cases had the uterus above 12 weeks of gestation and 280 grams. Logically, the rest 85-90% cases would not require a morcellation. The uterus up to 14-16 weeks sizes can be removed vaginally easily. Uterus size above the level of the true pelvis may be carefully attempted by experienced surgeons. However, a standby facility for conversion to LAVH or laparotomy is needed to deal with failure cases. It is not wise to attempt the vaginal hysterectomy on a uterus of above 20 weeks of gestation. Only 13.55% cases in our series required bisection and morcellation.Majority of uteri weighing less than 280 grams, did not require volume reduction maneuvers.
Techniques of volume reduction maneuvers during the vaginal hysterectomy
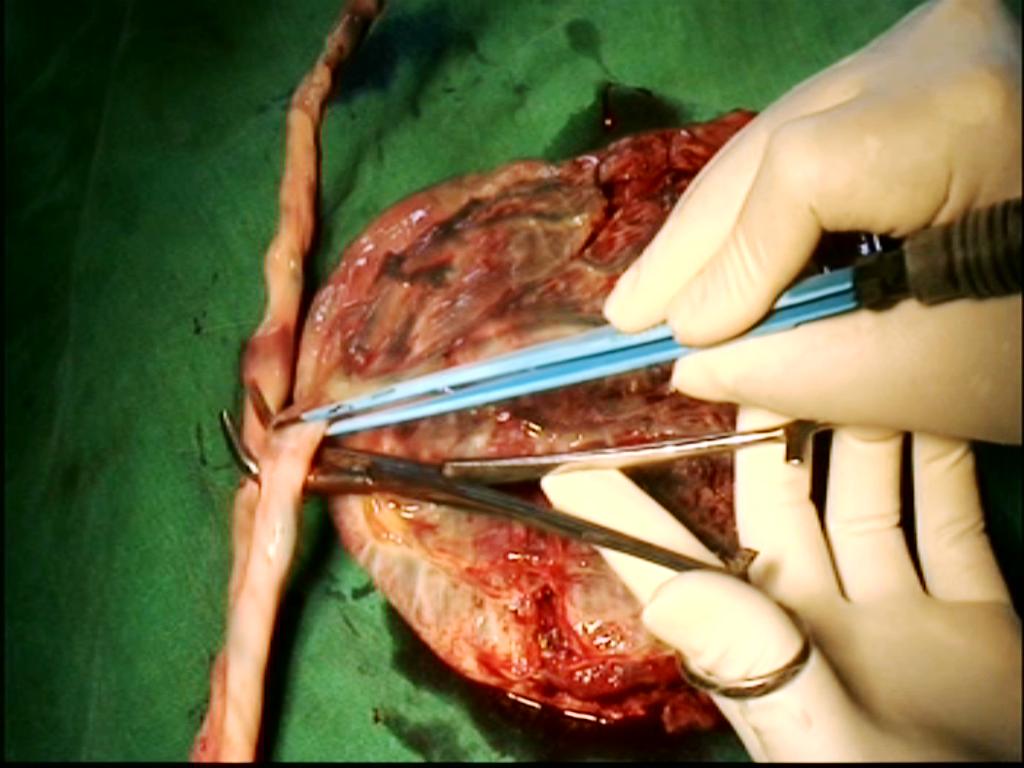
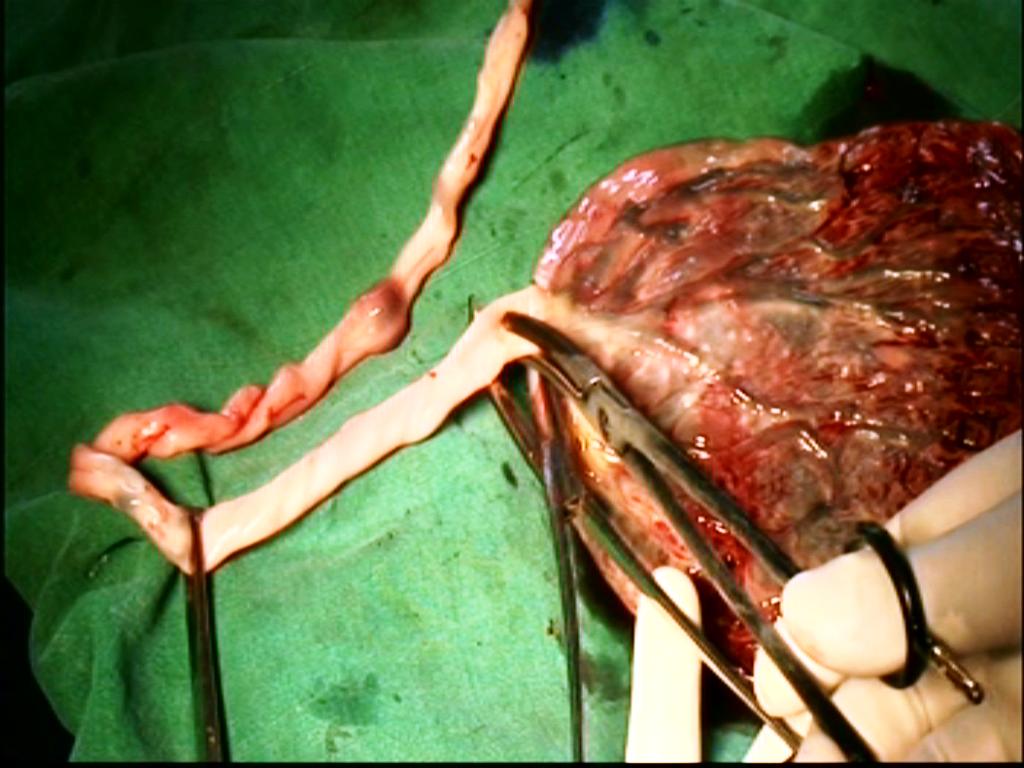
Bisection of the cervix, myomectomy of visible myoma, and wedge morcellation by knife and scissors of the directly visible bulk of the uterus are commonly practiced methods, and enough to minimize or remove the centrally occupying obstruction to the lateral pedicles. In our experience, generally, uteri weighing up to 300 grams do not require debulking. A soft uterus of 600 grams(Figure 5,6) has been removed intact by Purohit technique, for a right angle forceps can 'hook' a lateral pedicle from a tight working space, and brings it to the mouth of bipolar forceps and scissors.It is the largest reported uterus removed intact vaginally during the vaginal hysterectomy. Intraoperative indication of debulking:when no further lateral pedicle is 'hooked' on sweeping the tip of forceps around the expanded lateral wall of the uterus debulking is indicated.

Figure 5,6.(16 weeks size and 600 grams uterus removed intact by Purohit technique)
Only, 13.55% cases required volume reduction maneuvers when Purohit technique was used in contrast to more than 30% cases by conventional techniques. Lash procedure of intramyometrial coring is available for moderate size uterus and in a case with the suspected endometrial carcinoma, where, uterine cavity is kept intact. With the development of Purohit technique, a moderate size uterus may be removed intact thus, coring was not needed.
How to deal with the expanded lower segment
Volume reduction maneuvers are normally carried out after bilateral ligation of uterine arteries. Hemorrhage is expected in conducting debulking before ligation of uterine arteries in cases of large cervical polyp, big central cervical fibroid and requires the blood transfusion. Smaller ones do not cause problems thus can be attempted. Intracapsular morcellation of myoma removes the fear of injury to the neighboring tissues and reduces intraoperative bleeding.Cervical fibroid with uterus size up to 18 weeks size can be attempted by the Purohit technique.
How to deal with the expanded uterine fundus
Success of the debulking procedure depends on the successive descent of the uterus to the surgeon's view in response to the removal of wedges and traction. Solid single big firm myoma(>8cm) occupying above the level of the true pelvis and sitting above the brim does not descend adequately following morcellation and consumes lot of time, energy and patience. Soft cystic degenerated myoma following debulking responses well to the traction and descend faster towards the surgeon. A funnel type(pear shaped) below upwards expansion of the uterus is better for debulking than umbrella type(cannon ball shaped) expansion of fundus with a long stalk below. A big pedunculated fundal fibroid (>8cm size) with a long stalk some time does not come out with the uterus and often needs traction and debulking.Be careful when ultrasonography measures single fundal myoma of 8cm or more.Anterior fundal myoma of more than 8 cm remains away from the visibility, and a pelvic illuminator is usually needed.Posterior fundal myoma are better than anterior fundal myoma.
Conclusion
Thus, Purohit technique of the vaginal hysterectomy is a safe, effective technique in conducting vaginal hysterectomy and salpingo oophorectomy for almost all cases of benign disease of the uterus up to 18 weeks gestation size irrespective of preexisting conditions listed as the relative contraindications to the vaginal route excluding endometriosis. This technique promises the advantages of a high success rate, reduced need of laparoscopic assistance, low requirement of volume reduction, less intra and postoperative bleeding, mild postoperative pain,and early discharge from the hospital. Thus, reduce the cost and complications. The vaginal hysterectomy may be easier by adopting this newer technique using modern methods of hemostasis. Presently, if the ligature technique of hemostasis is replaced with the bipolar coagulation, and a right-angle forceps is used as a helper or anatomy delineator as in Purohit technique, then, the feasibility vaginal hysterectomy will be widely expanded. It will drastically reduce the number of abdominal and laparoscopic hysterectomies. The high feasibility rate of the vaginal hysterectomy (99%) in our study is due to the use of thin, long instruments like right angle forceps, bipolar forceps, pelvic illuminator, Purohit approach to uterine artery.
INTRAOPERATIVE COMPLICATIONS
Blood transfusion: Rarely required.
Be prepared for transfusion if the size of the uterus is more than 18 weeks and if the size of cervical fibroid is, more than 7-8 cm for it requires exhaustive morcellation, and sometime before ligation of at least one uterine artery.
Bladder injury It rarely occurs in cases with previous caesarean section.In our extraperitoneal technique of bladder separation from the cervix and anterior wall of the uterus, cystostomy is suspected when the finger enters in to a smooth empty space of bladder lumen and plenty of fluid floods the field on removal of the finger.Hold the incised margins and repair in 2 layers.
Rectal injury It occurs rarely in cases with dense rectum adhesion to cervix uterus following previous pelvic surgery or severe endometriosis. Intestine injury is usually avoided in the vaginal hysterectomy.
Ureteric injury It rarely happens during the vaginal hysterectomy due to carelessness of the surgeon while using thick bi-clamp or inserting needle deep in to the cardinal-uterosacral ligaments.
POSTOPERATIVE COMPLICATIONS:
Vault hematoma
We have seen in few cases during the early part of our study. A patient continues severe pelvic pain even after 48 hours. Ultrasonography of pelvis shows clot above vaginal vault.Vault hematoma has been minimized; by routine tracing of the incised edge of posterior leaf of the broad ligament up to the upper pedicles to check proper hemostasis, after routine use of our technique of vault closure and postoperative lavage of the pelvic cavity with Normal saline.No case of vault hematoma is seen after 2007.However, the vault hematoma is drained under transabdominal sonographic guidance after filling the bladder with about 300 ml normal saline.Best way to deal with pelvic hematoma is-go for three ports laparoscopy. Examine the pelvic cavity and stumps for hematoma. Do a lavage with normal saline. No cauterization is needed.
Burn injury to vulval skin and labia minora-Inner side of the vaginal skin and labia minora are occasionally trapped between the prongs of the activated bipolar forceps with broken insulation and are cauterized without the intention of the surgeon.This causes the superficial burn of skin. Thus, do not use bipolar forceps with broken insulation.Try to protect skin by lateral retractors. The patient with a small burn ulcer complains of burning sensation during micturation. It is treated with adequate amount of antibiotic ointment. Ask her to apply ointment before she intends to pass urine. It heals in few days spontaneously.
Bleeding from vaginal vault-
We have not seen postoperative bleeding from the uterine artery.Occasionally a phone call is received at the end of one month after operation saying, few drops of blood came out of the vagina.It usually comes from suture points of vault mucosa. It usually stops on its own. No treatment other than haemostatic drug is required. In 2 cases, we had to cauterize a tiny arteriole at the suture line of the vaginal vault to stop bleeding.In the second week, vault infection happened in few cases, They also complain of minimal vaginal bleeding.
Vaginal discharge:
It remains until suture materials are there at the vaginal vault. It stops on its own. No special treatment is required. Lavage of the pelvic cavity with Normal saline after closer of vaginal vault drastically reduces the fetid smell and thickness of the vaginal discharge.
Postoperative pyrexia occurs mostly due to cystitis.
Vault infection is rarely seen in the second week after operation.
Vault granulations rarely seen and are cauterized
Vault prolapse:
We have seen four cases of vault prolapse in the initial 680 cases before 2005. In all cases cystocele occurred with in one year of the vaginal hysterectomy. After 2005 and after adopting our technique of vault plication suture as described above, vault prolapsed has been minimized.
POSTOPERATIVE MANAGEMENT:
Routine prophylactic antibiotic, anti emetic (Ondansetron), Ranitidine IV fluid for 12 hours, Oral fluid started after 3 hours, Catheter removal after 12 hours, Vaginal drain (Ryle's tube) removal after 2-3 hours once the patient is shifted from the recovery room. Solid diet started after 12 hours, Injectable analgesic for minimum 12 hours then, oral analgesic. A patient can go home after 24-36 hours of operation, if she feels comfortable with oral antibiotics, analgesic, antacid and laxative, multivitamins. She is told to have mild vaginal discharge for few days, mild lower abdominal discomfort for few days. She is advised to contact over telephone, if any problem occurred.She may join work once she gains her confidence. Postoperative check up after 6 weeks. Anaesthesia during operation - we prefer mostly spinal anaesthesia
To watch the video, from You tube Purohit technique channel. To learn and practice, always watch the steps of the procedure before entering the operation theater for the vaginal hysterectomy at least for six months. Kindly see some interesting specimens removed during vaginal hysterectomy by Purohit technique and appreciate the scope of the technique. We request you to kindly fill up the feedback form or email your comments and suggestions on different aspects of the technique, which will be valuable for us.
Note:
We write for our readers to provide better services to our valued women clients. It is purely a social service and rendered free of cost. It has been a well-tried technique in our hospital. We have performed over 10000 vaginal hysterectomies by Purohit technique ( PTVH). It should be learned and followed accurately to get the best outcomes. The user and client purely decide the use of the technique
Declaration:
The authors and writers are not responsible for the legal problems arising out of the use of the procedures.
©All rights reserved with Purohit General Hospital and research center.
Updated as on date 30/05/2021
References
1
- Ram Krishna Purohit: Purohit technique of vaginal hysterectomy:
- a new approach BJOG (British Journal of Obstetric and Gynaecology):
- an International Journal of Obstetrics and Gynaecology, 2003 Dec, Vol. 110 (12) pp. 1115-1119
- View this document:To download right click and select save link as
2
- Ram K. Purohit: Purohit technique of vaginal hysterectomy:
- A new approach performed in 214 patients.
- Gynaecological endoscopy 2002 Dec; 11(6); 423-430
- View this document:To download right click and select save link as
3
- R. K. Purohit, A. K. Pattnaik:
- Vaginal Hysterectomy by Electrosurgery (An Extraperitoneal Approach),
- J Obstet Gynecol India Vol.51, No. 5: September/October 2001 Pg 162-164
- View this document:To download right click and select save link as
4
- Purohit Ram Krishna, Tripathy Prakash Narayan, Pattnaik Abhaya Kumar:
- Vaginal Hysterectomy Using Electrocautery and Purohit Approach To Uterine Artery,
- J Obstet Gynecol India Vol.53, No. 5: September / October 2003 Pg 475-478
- View this document:To download right click and select save link as
5
- Ram Krishna Purohit, MD, Jay Gopal Sharma, MS, Sarabjeet Singh, DGO, and Dipak Kumar Giri, MD:
- Vaginal Hysterectomy by Electrosurgery for Benign Indications Associated with Previous Cesarean Section
- JOURNAL OF GYNECOLOGIC SURGERY Volume 29, Number 1, 2013, Pages: 07 - 12 © Mary Ann Liebert, Inc.DOI: 10.1089/gyn.2012.0082
- View this document:To download right click and select save link as
6
- Ram Krishna Purohit, MD, Jay Gopal Sharma, MS and Shikha Joshi, MD:
- Adnexectomy During Vaginal Hysterectomy for Benign Indications Using Bipolar Hemostasis of Lateral Pedicles and Transvaginal Adnexa Mobilization
- JOURNAL OF GYNECOLOGIC SURGERY Volume 31, Number 2, 2015 Pages: 86 - 91 © Mary Ann Liebert, Inc.DOI: 10.1089/gyn.2014.0088
- View this document:To download right click and select save link as
7
- Ram Krishna Purohit, MD, Jay Gopal Sharma,Devajani Meher,Sanjay Raosaheb Rakh and Surya Malik:
- Completion of vaginal hysterectomy by electro surgery using anteroposterior approach in benign cases faced with obliterated posterior cul-de-sac
- View this document:To download right click and select save link as
8
- Dr.Ramkrishna Purohit,Dr.Jay Gopal Sharma,Dr.Devajani Meher,Dr.Sanjay Raosaheb Rakh,Dr.Minal Choudhary:
- A laparovaginal strategy to avoid bladder injury during laparoscopic-assisted vaginal hysterectomy in cases with ventrofixed uterus following previous cesarean section
- International Journal of Women’s Health
- View this document:To download right click and select save link as
9
- Ramkrishna Purohit, Jay Gopal Sharma, Devajani Meher, Mohammed Mahmoud Samy, Rupam Sarkar
- A Combined Strategy of Vaginal Hysterectomy by Electrosurgery with Post Hysterectomy Check Laparoscopy in Benign Indications Associated with Known or Suspected Concomitant Pelvic Disease: A Retrospective Study. PubMed, SCI, Scopus, ESCI, PMC indexed
- www.fortunejournals.com